
Ultrasound Evaluation of Abdominal Trauma in a Teenager
Posted on: June 7, 2017, by : Jeremy Root
Case:
A 17 year-old male presented to the ED after abdominal trauma. Prior to arrival, the patient was hit with a lacrosse stick to the right side of his back during a game. He felt immediate pain to his right flank and was removed from the game. He was taken to an outside hospital where the family was told he needed to have “emergency surgery” on his kidney. He was transferred to the pediatric ED in our tertiary care hospital. The patient received one dose of morphine and Zofran prior to arrival.
ROS: negative
PMH/medications: none
Physical Exam:
T 36.3 HR 60 RR 24 BP 112/72 SpO2 100%
The patient was alert and cognitively intact with pain on movement. There were no abrasions or bruising. He had normal capillary refill. Lungs were clear bilaterally and he moved all extremities without pain or difficulty. His abdomen was soft and non-distended with diffuse tenderness to palpation and mild guarding. He was severely tender on the right flank with notable guarding, no tenderness on the left flank. He had no spinal tenderness or step-offs.
OSH labs showed normal hemoglobin and hematocrit.
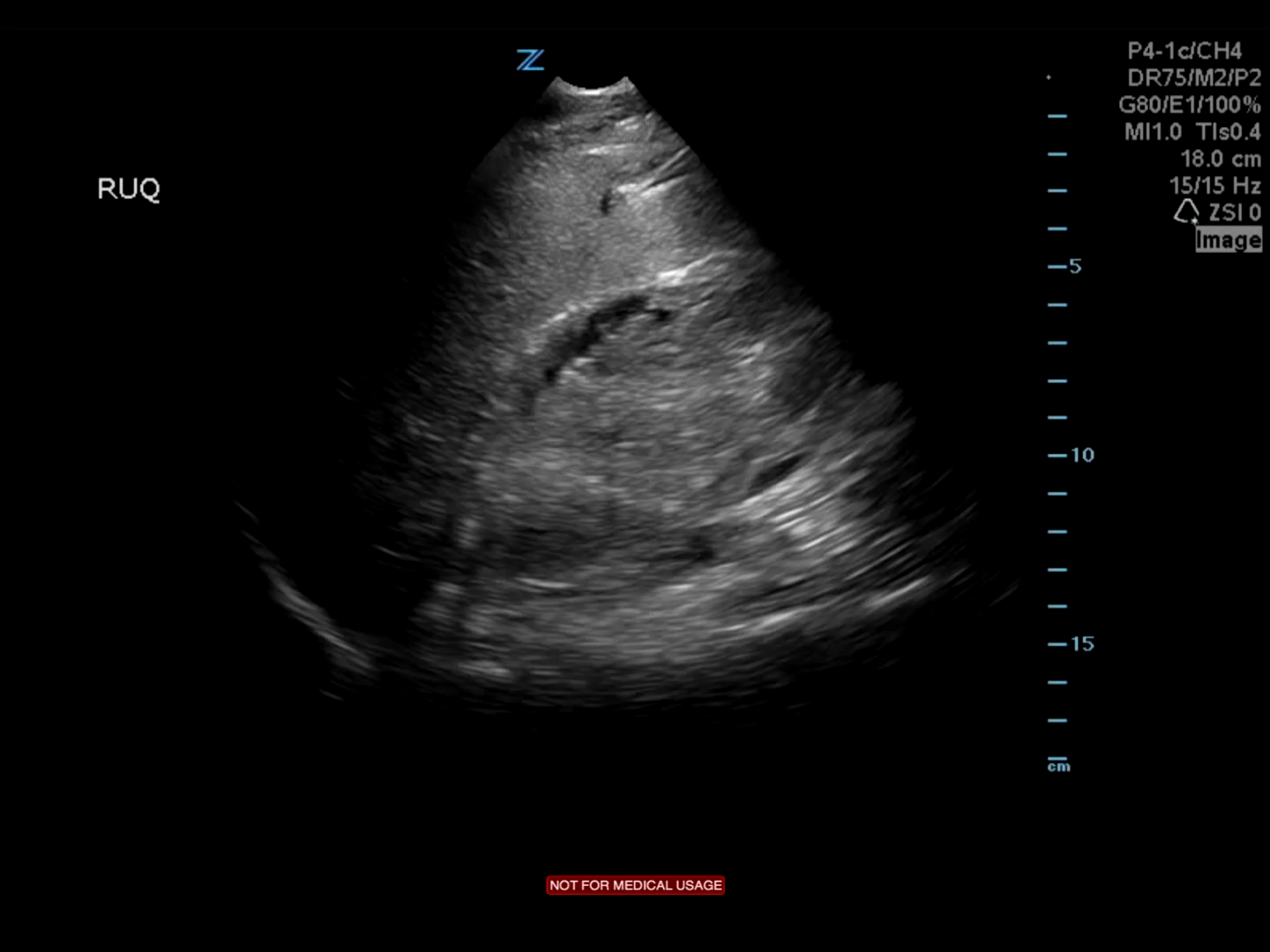
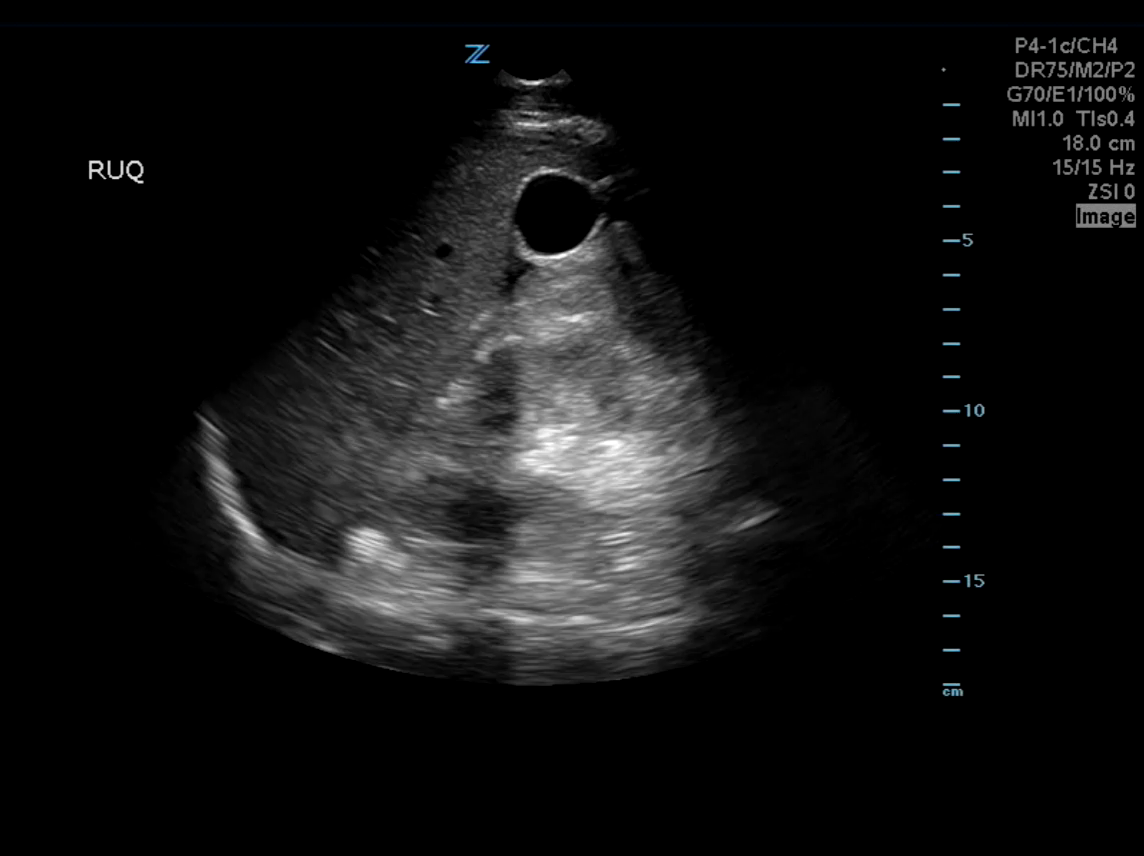
Point-of-care ultrasound (POCUS) findings: Liver and Right kidney.
Bedside interpretation:
Video 1:Renal parenchyma severely distorted.
Video 2: Small perihepatic free fluid.
ED Course:
Patient was noted to be hemodynamically stable and his pain was controlled with IV narcotics. Trauma surgery was consulted to review the OSH CT Abdomen/Pelvis.
Radiology interpretation of OSH CT scan: Right sided Grade 5 renal laceration according to the AAST (American Association for the Surgery of Trauma) injury scoring scale. Small (less than 1 cm) liver laceration in the lowermost aspect of the segment VI.
Discussion:
Patient was admitted to the trauma floor and urology was consulted. Hemoglobin and hematocrit (H&H) were monitored closely and patient began to drop his H&H on hospital day 4. Also on hospital day 4, the patient was taken to the OR by urology for stent placement and clot evacuation. Nephrology was consulted for hypertension believed to be secondary to a perinephric hematoma compressing the kidney and was patient was placed on blood pressure medications.
The kidneys are more susceptible to injury in children than adults due to the pediatric kidney’s relatively larger size in a child’s abdomen and pelvis.[1] According to the AAST grade V renal injuries are consistent with a shattered kidney, avulsion of the renal hilum, uretetopelvic avulsions, or complete laceration of the main renal artery or vein (Figure 1).1,[2],[3]


The management of high-grade blunt renal trauma has evolved. In the past, severe renal injuries were treated with immediate surgery, which was thought to improve renal salvage rates, reduce morbidity and lessen the likelihood of secondary exploration.[4] Indications for surgery included perirenal hematoma, extrarenal extravasation on intravenous pyelography (IVP), hemodynamic instability and pedicle injury.1,[5] Recently delayed operative management or nonoperative care has been recommended for higher grade renal injuries to allow for clinical
[1] Fraser JD, Aguayo P, Ostlie DJ, Peter SD. “Review of the evidence on the management of blunt renal trauma in pediatric patients.” Pediatr Surg Int. 2009. 25:123-32.
[2] Gaillard AF, et al. “AAST kidney injury scale,” Radiopaedia. https://radiopaedia.org/articles/aast-kidney-injury-scale. Accessed May 17, 2017.
[3] Runyon MS. “Blunt genitourinary trauma: Initial evaluation and management.” UpToDate. https://www.uptodate.com/contents/blunt-genitourinary-trauma-initial-evaluation-and-management. Accessed May 18, 2017
[4] “Case AS. “Blunt Renal Trauma in Children.” J Trauma. 1983, 23:123-7.
[5] Van Ahlen H, Bruhl P, Porst H. “Pediatric blunt renal trauma—surgical or conservative management?” European Urology. 1988, 14:407-11.
[6] Ahmed S, et al. “Renal Parenchymal Injuries Secondary to Blunt Abomdinal Trauma in Childhood: A 10-Year Review.” Br J Urol. 1982, 54:470-7.
[7] Wessel LM, et al. “Management of kidney injuries in children with blunt abdominal trauma.” J Pediatr Surg. 2000, 35:1326-30.