
AOTW: Sport-Related Concussion in Children and Adolescents
Posted on: September 1, 2014, by : Lenore Jarvis MD MEd
Unfortunately concussion is a common diagnosis, especially in the fall with the initiation of football season. Thankfully, the AAP released a great article summarizing current concussion guidelines. Highlights from this article are found below.
Halstead, Mark E., Walter, Kevin D., THE COUNCIL ON SPORTS MEDICINE AND FITNESS,
Clinical Report–Sport-Related Concussion in Children and Adolescents
Pediatrics 2010 0: peds.2010-2005
Intro: brains are still developing and may be more susceptible to the effects of a concussion
Definition: a complex pathophysiological process affecting the brain induced by traumatic biomechanical forces and includes 5 major features:
1. Caused either by a direct blow to the body with an “impulsive” force transmitted to the head.
2. Results in the rapid onset of short-lived impairment of neurologic function that resolves spontaneously.
3. Acute clinical symptoms largely reflect a functional disturbance rather than a structural injury.
4. May or may not involve loss of consciousness (LOC).
5. No abnormality on neuroimaging studies.
Epidemiology: 300,000 sport-related concussions occur each year, up to 3.8 million recreation & sport-related. 8.9% of all high school athletic injuries. Girls higher rates than boys. Football>soccer>basketball.
Signs & symptoms: HA most frequent. LOC in <10%.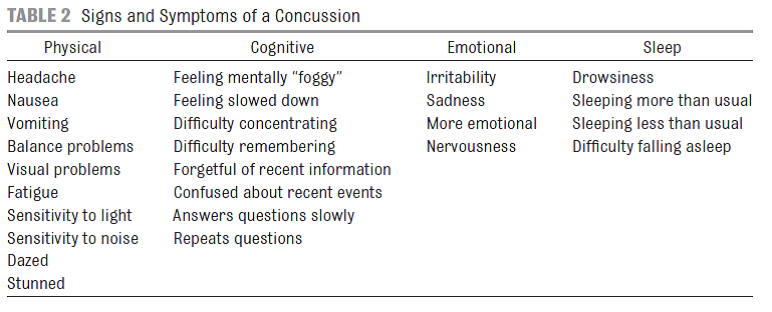
Initial Assessment: On the field: ABCs + stabilize the C-spine. Symptoms, neuro exam, cognition. Sideline assessment tools are available.
Office/ED: thorough history, including signs and symptoms as well as details of any previous head injuries; head and neck examination; neurologic examination, including gait and balance assessment; and assessment of cognitive function. Monitored for any deterioration of condition. If concern for a structural brain abnormality, neuroimaging should be considered.
Conventional neuroimaging is typically normal in a concussive injury.
• Signs and symptoms worrisome for more serious injury include severe headache; seizures; focal neurologic findings on examination; repeated emesis; significant drowsiness or difficulty awakening; slurred speech; poor orientation to person, place, or time; neck pain; and significant irritability. Patients with LOC for more than 30 seconds.
• CT is the test of choice during the first 24 to 48 hours after injury
• MRI is more appropriate 48 hours or longer after an injury
• Functional neuroimaging will likely provide a more accurate picture of the injury and may help predict recovery better than structural neuroimaging, but further research and wider availability is needed
Neuropsych testing: a means to provide an objective measure of brain function
• does not independently determine if an athlete has experienced a concussion or when he or she may safely return to play
• ideally a baseline or preinjury test should be obtained – many teams and schools will administer tests
• if an athlete is suffering from postconcussive symptoms over several months or has had multiple concussions, formal assessment by a neuropsychologist may be beneficial, specifically to identify areas for which the athlete may need academic accommodations.
Management: The athlete should not be allowed to return to play that same day!!! Avoid activities and situations that may slow recovery.
There is currently no evidence-based research regarding the use of any medication in the treatment of the concussed pediatric athlete.
• It is commonly recommended that NSAIDs or aspirin be avoided immediately after a suspected head injury for fear of potentiating the risk of intracranial bleeding. This remains more of a theoretic risk.
Before considering a return to play, any medications used to reduce symptoms must be stopped and the athlete must remain symptom-free off medication.
Cognitive rest: concussion is a functional rather than structural injury of the brain
• Temporary leave of absence from school, shortening of the athlete’s school day, reduction of workloads in school, and allowance of more time for the athlete to complete assignments or take tests
• Communication with school nurses, administrators, and teachers to be sure they understand these recommendations
• Activities that require concentration and attention (playing video games, using a computer, and viewing TV) may exacerbate symptoms
• May need to avoid driving temporarily due to slowed reaction times
Physical rest: broad restrictions of physical activity should be recommended
Return to play: No athlete should return to play while still symptomatic at rest or with exertion. Often need stepwise return to play.
• Although the vast majority of athletes with concussion will become asymptomatic within a week of their concussion, numerous studies have demonstrated a longer recovery in younger athletes.
Follow recovery with postconcussion symptom scale.
Long-term Effects:
• persistent deficits in processing complex visual stimuli
• athletes with 2 or more concussions demonstrate statistically significant lower grade-point averages