
Hot Seat #43 Denouement: 15 yo with a neck mass
Posted on: September 25, 2014, by : Lenore Jarvis MD MEd
by Adam Kochman, Inova Children’s Hospital
with Karen O’Connell, Children’s National
The Case
15 y/o previously healthy male referred form PCP office with 4-5 weeks of right neck mass. The challenge of this case involves the diagnostic work-up for a neck mass. For a complete case presentation with audience and Hot Seat Attending comments, please click here.
Here’s How You Answered Our Questions
Fellows and attendings seemed to be in agreement on this one! Although, not everyone would have obtained a neck XR, most would order an additional neck image with the initial work-up. The concern was that the mass has “indiscrete borders, is nonfluctuant and immovable.” Most would use an ultrasound as a starting point as it does not involve radiation. Dave states that, “I try to do neck CT’s almost never in kids older than 5.” Paul mentions that an ultrasound is a good starting point, but one should expect to need additional imaging. Several attendings mention that they would use the ultrasound to help guide further imaging: CT vs CTA vs MRI vs MRA.
Denouement
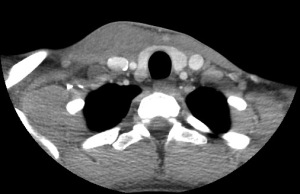
CT scan demonstrated abnormal right SCM with focal abnormal enlargement measuring ~21mm, minimal heterogeneity without encapsulated abnormal fluid collection. Heme/Onc was consulted in the ED and decision to obtain MRI which demonstrated an ill-defined infiltrative lesion of right SCM with extensive heterogeneity. No evidence of LAD.
Given pt overall well clinical appearance, stable vitals and no evidence of airway compromise, ultimate decision made in conjunction with Heme/Onc attending was to discharge home from the ED and f/u in Hematology clinic in 2 days.
At Hematology clinic visit 2 days later, there was interval increase in tenderness and erythema of overlying skin. Neck movement more limited secondary to pain but pt remained afebrile and well appearing. With suspicion for associated bacterial infection (possibly secondary to underlying mass), the patient was started on oral Clindamycin and referred to ENT-oncologist for open biopsy in 3 days.
Pt returned to ED 48 hours later with increased pain and erythema and acute onset significant purulent drainage. Repeat CT obtained demonstrated interval increase in soft tissue swelling and inflammation at right SCM, now measuring 7.9 x 4.7cm with new fluid collection extending to skin surface.

Pt was taken to OR by ENT where extensive purulent drainage was suctioned and sent for culture. The SCM and all surrounding tissue was indurated and very hard with some necrotic portions. Small cyst-like structure removed and sent for pathology.
Culture ultimately grew out Strep intermedius and Eikenella, CT images re-examined and in concurrence with operative findings, diagnosis of infected branchial cleft cyst was made. All pathology returned negative for malignancy. Anaerobic, fungal and AFB cultures all negative. Pt received IV Ceftriaxone on floor for 3 days and was subsequently discharged home on Augmentin with ENT f/u.
Debrief Teaching Points – from Thursday Conference
1. Imaging: XR as applicable, but ultrasound is a good start to “get an idea of what you are dealing with.” Then consider a CT, CTA, MRI, MRA, etc. If you think an excisional biopsy may be warranted, consider discussion with Surgery to help the decision on imaging modality.
2. DDX: inflammatory, congenital, neoplasm, traumatic. A good physical exam dividing the neck into 3 parts can help aid in your diagnosis: anterior triangle, midline, posterior triangle.

4. Labs: CBC, ESR/CRP, uric acid/LDH, CMP may help guide management. Don’t forget ppd, as appropriate. Consider EBV, CMV, HIV & B henselae.
3. Bonus: from AAFP.org
