
Hot Seat #49 Denouement: 8 y/o respiratory distress and wheezing
Posted on: January 22, 2015, by : Lenore Jarvis MD MEd
by Fareed Saleh, Children’s National
with Karen O’Connell, Children’s National
The Case
8 y/o F bounce-back to the ED for respiratory distress, wheezing and facial swelling after being discharged 1 day prior with a diagnosis of LUL pneumonia and asthma exacerbation. The challenge of this case is how to manage the increasing worsening distress while determining the cause of the distress.
Here’s How You Answered Our Questions
PEM fellows/providers would likely simultaneously rethink the asthma diagnosis while increasing respiratory support for the patient. Next steps for both groups involve obtaining a CXR and thinking about positive pressure ventilation given significant tachypnea. At this time, we are unsure of the diagnosis. Several providers state that in a sick patient, especially one not responding to treatments, one could think about giving vancomycin. After more information has been obtained and a diagnosis has been established, antibiotic therapy can be tailored.
Denouement
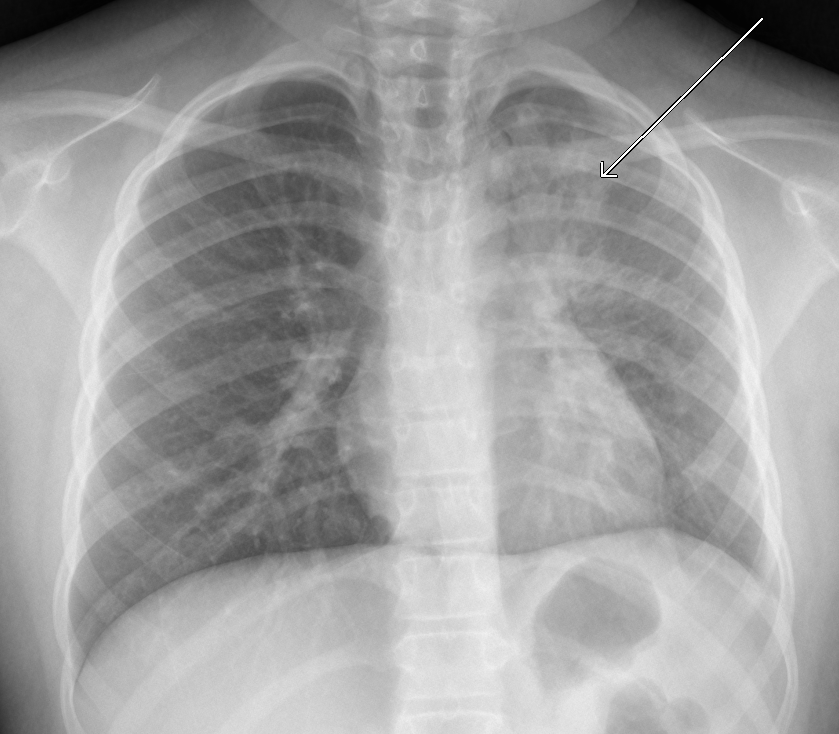
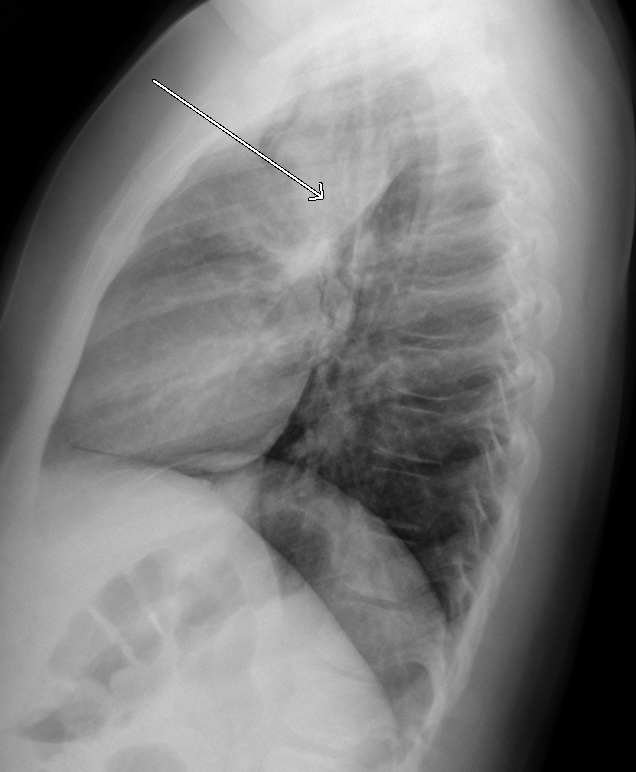
A repeat CXR was done showing pneumomediastinum that tracked up to the patient’s cheeks. Pt was subsequently placed on NRB and admitted to PICU. On HD #2, pt was placed on BiPAP given worsening respiratory distress with antibiotic coverage broadened to include azithromycin and vancomycin. Pt was successfully weaned from BiPAP to RA by HD #4 and discharged home without incident on HD #5.
Teaching Points from Thursday Conference
“You are surrounded by assassins – trust no one!” When things don’t make sense, ensure you rethink from the start. If you have an “asthmatic” that is not responding appropriately to treatments, broaden your differential. Obtain a CXR, EKG, etc.
Interesting that the child tolerated the BiPAP without worsening the air leak.