Hot Seat #70: 14 yo F w/ continued low-grade fever and cough
Posted on: March 1, 2016, by : Jared Friedman
Jared Friedman MD, INOVA Children’s Hospital
with Jennifer Chapman MD, Children’s National Health System
The Case
14 yo F history of mild intermittent asthma presented to the Peds ED with continued low-grade fever and cough x 1 week.
Timeline of Events:
Day 1: Patient with sore throat, runny nose, and low grade fevers.
Day 3: She presented to her PCP at day 3 with same symptoms = negative rapid strep – culture pending.
Day 5: Throat culture returned positive for strep pharyngitis – started on Amoxicillin. Also had worsening cough – started on QVAR, Albuterol PRN, and Prednisolone.
Day 7: Continued to have cough and low-grade fever despite being on Amoxicillin (Day 3/10) and QVAR, Prednisolone, and Albuterol PRN – went to Peds ED.
ROS: Patient and parents deny nausea, vomiting, headache, chest pain, abdominal pain, difficulty breathing, shortness of breath, travels, sick contacts, or any other concerns.
FHx: Two siblings with asthma.
Allergies: Pollen, apples, pears, cherries, peaches, and bean sprouts
PE Day 7: Triage VS in Peds ED: BP105/69, HR120, T99.2, RR16, O297% RA
General: awake, alert, nontoxic, and comfortable
HEENT: Posterior OP normal, TM normal b/l, normocephalic, mucous membranes moist
Eyes: Lids normal, no conjunctival injection
CV: Tachycardic and normal rhythm, no murmur
Lungs: Diminished BS left and upper right, no work of breathing
Abdomen: Soft, no masses or distention, nontender
MSK: Upper and lower extremities warm and well perfused, no edema or evidence of trauma, neck exhibits FROM by observation
Skin: Warm and diaphoretic, no rash
Neuro: Moving extremities symmetrically and well by observation, no focal weakness
Psych: Normal behavior and developmentally appropriate
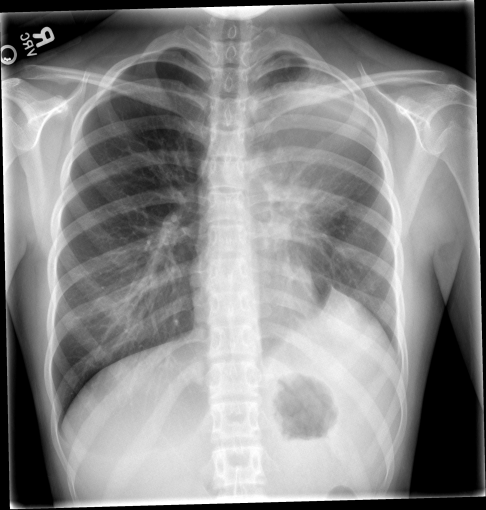
Screening blood work and CXR:
CBC: 7.74, 14.7/44.2, 324 86% Neutrophils, 0% Bands, 9% Lymphocytes, 4% Monocytes
Blood Culture: Pending
CMP: 138/4.3, 104/23, 9/0.8, 130
CRP: 28.5
Questions for you:
Update:
Patient was diagnosed with LUL PNA, given Ceftriaxone x1, NS Bolus x1, and discharged home on Augmentin to be followed-up by the PCP in the Office the next day.
The patient did not follow-up with the PCP the next day, but instead did so three days later when she developed a rash.
Day 10: On Augmentin at home, she was still having fevers (TMax 102F), but now she developed a rash on her chest that was spreading to other parts of her body. The PCP switched her to Cefdinir and told her to follow-up as needed.
Day 13: Continued on Cefdinir, but had worsening cough (pain near clavicles with coughing), URI symptoms, and still febrile (TMax 102.5F), so she went back to the Peds ED.
ROS: Patient and both parents deny any nausea, vomiting, headache, chest pain, difficulty breathing, shortness of breath, travels, sick contacts, or any other concerns.
PE Day 13: Triage VS in Peds ED: BP98/55, HR101, T103.8, RR22, O296% RA
General: Alert, tired-appearing, but uncomfortable shivering and intermittently coughing during exam, NAD talking to both Parents in bed
HEENT: PERRLA – no injected conjunctiva. No photophobia. MMM. Clear PO without exudate/petechiae. Neck supple – FROM throughout.
Lungs: Decreased BS in left lower lung field with intermittent rales and crackles. Good aeration otherwise on right side. No wheezes/flaring/retractions.
CV: Tachycardic, RRR, +2 pulses b/l
Abd: Soft abdomen, ND. No HSM. Mild non-specific abdominal pain (R>L). No rebound/guarding.
Skin: WWP, CR erythematous, blanching blotch-like rash on chest, abdomen, and neck
MSK: Moves all extremities b/l
More questions:
Repeat blood work and CXR:
CBC: 17.54, 14.9/45.4, 222 83% Neutrophils, 0% Bands, 8% Lymphocytes, 9% Monocytes, 1% Eosinophils
Blood/sputum/RVP culture: Pending
CMP: 136/4.2, 103/24, 8/0.7, 92/8.5, AST/ALT 25/76, ALKP 125, Alb 2.7, TPROT 7.3, TB 0.8
ESR: 143
CRP: 28

A CT is obtained:

One more question:
How would you approach this case? Please share your opinions by clicking on “What do you think?” below.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
The initial CXR had abnormality in the LLL as well as LUL opacity. that’s not a normal looking left hemi-diaphragm although doesn’t look like a hernia or hemi-paresis, so not sure what that is. Unless I’m wrong and that’s a weird normal variant, but that would be good to know 🙂
The whole reason to do a CXR in a kid who has a clinical pneumonia is to look for stuff like this (effusion, cardiomegaly, mediastinal mass, empyema, fungal ball, etc)….not to diagnose a simple pneumonia. So assuming that’s not a normal variant in the LLL, the time to act was on Day 7 when there was a very abnormal CXR. That would’ve been a good time to get radiologic clarity on the CXR findings and consider chest CT.
No eosinophilia is reassuring that it’s not aespergillosis/ABPA, but I can’t say I’m an expert interpreting chest CT’s and would defer to the radiologists to help us decide if that’s a mass or if it’s more infectious with rim-enhancing features concerning for fungus or abscess.
radiologists are your friends 🙂
unless they tell you that a clinical correlation is recommended.
Agree with Dave on the Day 7 miss. Although, in our dimly lit worlds with fuzzy screens, in a packed waiting room, I could see maybe missing it…. but hopefully not. One key I’ve learned when head scratching a chest film is to cover up the bottom half of the film and then the top half. This tends to “highlight” in your mind the asymmetric findings on CXR – like in that LUL. Also, is that axillary LAD on both sides that is seen on both xrays? There shouldn’t be anything in the pits normally on CXR, so when I see fullness, I think of TB, next thing I think about is TB, then HIV/cancer/lymphadenitis/catscratch.
Most likely LUL mass vs fungus vs enlarged hilar lymph nodes (from TB); with subsequent “collapse consolidation” of a LLL subsegment. Definitely talk to radiology for chest CT, then someone post-admission needs to grab a piece of tissue for pathology and cultures workup – either surgery and/or pulm for a bronch.
Well, she didn’t follow up to plan, and I could see progression of illness resulting in the story outlined above. Could we have changed things on Day 7? With the funny looking diaphragm, I may have started with an ultrasound to rule out effusion, since she was still hemodynamically stable, and then going to CT depending on what that showed. ?lingular involvement there? By the time she returned, the Upper lobar opacification would warrant a rule out for a post-obstructive process. Her follow up was not exactly as one would have hoped, and it would be interesting to know what the PCP was thinking at the clinic.Rash is concerning? add legionnaires to differential?
I am also curious about the asthma history and whether steroids would put the patient more at risk for a fungal infection. Looking forward to hearing what happened.
To summarize, this is a 14yo girl with mild intermittent asthma who presents with a week of cough, sore throat, low-grade fevers. Symptoms are continuing after 3 days of amoxicillin for strep + throat swab.
To start, work on a differential diagnosis. Shilpa’s favourite mnemonic is SPIT:
Serious: Lemierre’s is indolent, causing sore throat, low-grade fever, progressing to neck pain/swelling and effects of septic emboli (HA, difficulty breathing, cough, sepsis); peri-tonsillar abscess, but patient has a symmetrical pharyngeal exam and improving sore throat (I think); TB: no known risk factors, no night sweats, no weight loss; fungal infection: again, no reason to suspect patient is immunocompromised (not on chronic steroids).
Probable: bacterial pneumonia; atypical pneumonia, including Mycoplasma and Chlamydia (>> Legionella); influenza, though would expect high fevers; rhinovirus, adenovirus, human metapneumovirus.
Interesting: usually same as serious- Lemierre’s: want a good history and exam of the neck, for focal tenderness, swelling, limitation of movement, pain with swallowing.
Treatable: pneumonia.
ED course #1: the work-up shows elevated segs with a normal white cell count and high CRP. The CXR shows an elevated L hemi-diaphragm with haziness in the LUL. This suggests volume loss, though the Xray doesn’t show obvious atelectasis. Could there be obstruction as suggested in earlier post (LNs, foreign body).
The decision on next steps begins with her overall appearance and likely diagnosis. She is not toxic appearing, though her HR of 120 needs focus and attention. Other considerations: if pneumonia is my most likely diagnosis (though again, the CXR confuses me a bit and I would discuss with the Radiologist), then I need to decide if she falls into the category of failed outpatient treatment: fever persisting longer than 48 hours, increasing symptoms, or worsening CXR. I am not clear from the information provided if the patient meets the first 2 criteria.
On her return visit, she has persistent and elevated temps, tachycardia, and worsening respiratory symptoms. The CXR shows a significant consolidation in the LUL with round fullnesses at the hilum, that I would discuss with the Radiologist. The chest CT shows a consolidation posteriorly, so don’t think it is a malignancy (pt is old for neuroblastoma). So likely this is an infectious process.
What can be done next:
– Admit on increased Strep pn coverage: ceftriaxone and Vancomycin;
– Consider addition of azithromycin;
– Fungal coverage: not yet.
– Respiratory panel to get a snapshot of whether influenza is now added in;
– Careful travel hx and exposure hx for TB and unusual bacterial infections;
– HIV screen; TB testing (quantiferon gold);
– Does she need to have bronchoscopy to image the upper lobe bronchus and collect sample.