
Hot Seat Case # 109: 16 year old male with a chronic cough
Posted on: March 16, 2018, by : Hilary Ong
Hilary Ong, MD Children’s National Medical Center
with Ioannis Koutroulis , MD Children’s National Medical Center
16 year old male with asthma and perinatally acquired HIV on antivirals who presented with a chronic cough that began a few months ago. The cough is sometimes productive with yellow mucous but often is a dry nonproductive cough. The cough is worse in the morning and at night, and is associated with sore throat and nasal congestion. The patient denies alleviating factors and reports albuterol exacerbates the cough. He has had intermittent subjective fevers. He is poorly compliant with his medications and cannot recall his last CD4 count despite it being checked recently. He was treated in the ED 2 weeks ago for asthma and seasonal allergies. His symptoms improved initially for a few days, but worsened again.
ROS:
Constitutional symptoms: subjective fever, denies chills, denies fatigue
Skin symptoms: denies rash
ENMT symptoms: sore throat, nasal congestion
Respiratory symptoms: cough, denies shortness of breath
Cardiovascular symptoms: denies chest pain
Gastrointestinal symptoms: no abdominal pain, no vomiting, no diarrhea, no constipation
Genitourinary symptoms: no dysuria, no hematuria, no discharge
Musculoskeletal symptoms: no muscle pain
Neurologic symptoms: no headache, no dizziness, no weakness
PMH: HIV, asthma
Medications: albuterol, fluconazole, levofloxacin, Combivir, Bactrim, and Zyrtec
Social Hx: unknown TB contacts
Vital signs: T:37.8 HR:118 BP:118/71 RR:20 O2:98%
General: Awake, alert, well appearing
Skin: Warm. Dry. Intact. No pallor. No rash.
Eyes: PERRL, EOMI, Normal conjunctiva, no scleral icterus
Ears/nose/throat: Normal TM’s bilaterally, no effusions. MMM, no pharyngeal erythema or exudates
Neck: supple, full ROM. no LAD.
Heart: Tachycardic, regular rhythm, no gallop or murmur, strong pulses.
Lungs: Diffuse I/E wheezing with scattered crackles bilaterally. Good aeration bilaterally with symmetric chest rise. Tachypneic with mild subcostal retractions.
GI: Soft, Normal bowel sounds, Abdomen distended, No HSM.
Neuro: Alert, non-focal exam.
His repeat vitals were T 37.8 HR 125 BP 124/88 Sat 91% RA (30mins after albuterol)
Labs are as shown below:
WBC 2.01, Hg 9.2, Hct 28.4, Plt 189 136/3.9/104/24/9/0.62<131
74% Neutrophils AST/ALT 253/115, ALK 291
13% Lymphocytes TP 5.5, albumin 1.0, Bili 0.3
10% Monocytes
Blood culture: negative gram stain
CD4 and HIV viral load pending
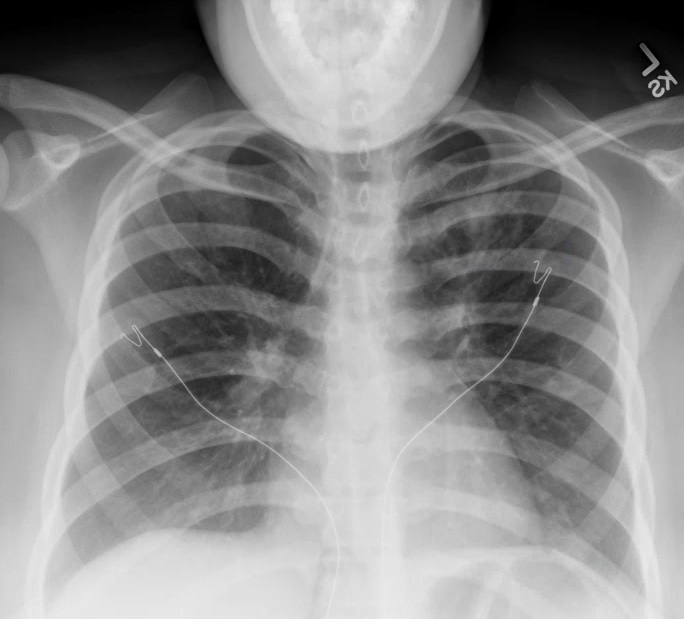
CXR as shown below:
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
This is a case of a chronic cough in a young man who may be immunocompromised, with findings of wheezing and retractions on exam. Given the adequate treatment for asthma and prolonged symptoms, asthma is unlikely to be the full diagnosis. Thinking of infections, bacterial pneumonia is unlikely (prolonged symptoms, non-focal exam and CXR, absence of fever). While viral and atypical pneumonias are possible, the timecourse again seems long. Even without concern for the immune system, acquired fungal infections and TB can cause sub-acute symptoms. Thinking of HIV-specific conditions, he is not ill enough for PJP to be a primary concern, but should be kept in mind. My last thought is of LIP, an interstitial pneumonitis associated with autoimmune conditions and with HIV.
For this patient, a call to ID and a chest CT prior to admission. He may need bronchoscopy in-hospital.
You are going to have a difficult time sending this patient home. He was tachycardic on arrival and not surprisingly persistently tachycardic after the addition of an albuterol neb. Furthermore he has borderline O2 sats (maybe some improving V/Q mismatch post alb…). The only way this patient could potentially and safely go home is after observation to confirm he does require O2, confirming his HR returns to normal range and with an ID c/s and plan in place for close outpatient follow up. Based on the story I would err on the side of caution and probably push for admission with an ID c/s and discuss with them the indication for chest CT.
I agree Jeremy..Too risky to discharge considering VS and symptomatology..A chest CT would probably be warranted although I’d want to know his CD4 count and viral load because specific opportunistic infections are strongly correlated with those numbers.
Agree with everything noted above. The other thing I’d want to do is talk to radiology over the phone about the CXR – is there concern for Kaposi Sarcoma in this patient given his complaint of cough and what may be some fullness in the perihilar regions bilaterally? Of course, this would be much better clarified on the chest CT that the other fellow and attendings are recommending.