
Hot Seat Case # 114: 2 week old with bloody stools
Posted on: June 11, 2018, by : Haroon Shaukat MD
Rachael Batabyal, MD Children’s National Medical Center
with Christina Lindgren , MD Children’s National Medical Center
2 week old ex-FT F presents as referral from PCP’s office with 1-2 days of hematochezia and 2 episodes of non-bloody, non-bilious emesis. She has had >10 stool diapers in the last 24 hours, mostly watery consistency though 1-2 of them with hard balls of stool. Parents noted gross blood in each diaper change. She has been afebrile with a Tmax of 99 rectally at home. She was referred from the PCP’s office for concern for abdominal distension and hypotonia. She has had decreased feeding at home (only 2 bottles in the last 12 hours), but she took a full bottle on the way from the PCPs office. She is formula fed. She has had no URI symptoms. No sick contacts. No recent travel.
Parents show you multiple pictures of diapers with watery stools and gross blood.
Birth Hx: ex FT F, C-section for maternal anatomy (narrow pelvis), No NICU stay. No postnatal complications. Family states patient stooled multiple times in the first 24 hours of life. She has regained her birth weight.
Fam Hx: No relevant family medical history
Surgical Hx: No surgeries
Meds: None
Allergies: None
ROS is notable for no fevers, no weight loss, no URI symptoms, positive for vomiting, diarrhea, and decreased feeding.
Vital Signs: T: 37.3, HR: 136, RR: 34, BP: 82/56 SpO2: 100%
Gen: Well appearing, alert, no acute distress
Skin: Warm, dry, intact, no rashes, no pallor
HEENT: AFOF, PERRLA, oral mucosa moist
CV: Regular Rate and Rhythm, no murmurs, rubs, or gallops, 2+ femoral and DP pulses, cap refill <2 seconds.
Resp: Clear to auscultation bilaterally, symmetric chest rise, no tachypnea
GI: Distended, soft, non-tender, normal bowel sounds, no organomegaly
GU: Normal female anatomy, no anal fissures appreciated, gross blood visible in the diaper.
Ext: No swelling, no deformities, normal ROM
Neuro: awake, alert, PERRLA, normal tone, symmetric moro reflex b/l, moving all extremities
Her FOBT was positive and upon re-examination, her abdomen appeared more distended. Repeat VS were T 37.8, HR 160, BP 80/50, RR 46, SpO2 100% on RA. She was refusing the bottle and had 6 additional bloody stools. Parents stated she was not acting like herself and seemed sleepier.
An abdominal X-ray was performed and is shown below:

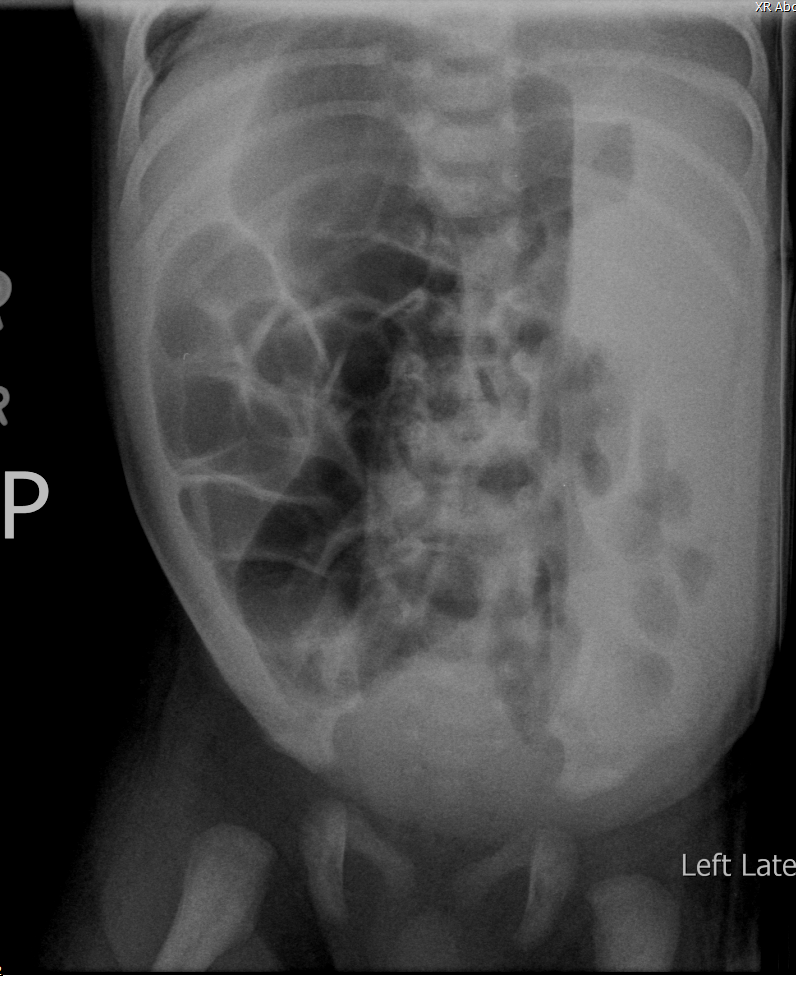
Labs: CBC: 7/15/44/346, 10% bandemia, I:T ratio: 0.65. BMP is unremarkable. Blood Glucose was wnl.
At this point surgery was consulted who recommended an Upper GI as well as a barium enema. The barium enema was concerning for long-segment Hirschprung’s disease. A full sepsis workup was completed.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
It is important to first consider if this is a brisk upper GI bleed versus a true lower GI bleed. It is unlikely to be an UGI bleed given that this infant is not toxic appearing and has had no coffee ground emesis. One could consider placing a NG tube to rule out an UGI bleed, though to be honest I have never done this in an infant and placing a NG tube for gastric lavage is no longer recommended. So, assuming this is most likely a LGI bleed based on the patient’s appearance you have to consider your differential which in my mind includes: infectious colitis, allergic colitis, swallowed maternal blood, anal fissures, necrotizing enterocolitis, malrotation with midgut volvulus, coagulopathy and hirschsprungs with associated enterocolitis. A few other things that are very uncommon in the neonate but worth considering on your differential would be: vascular malformations, a gastrointestinal duplication cyst and Meckle’s diverticulum.
Thinking through this differential can help guide your management moving forward. Swallowed maternal blood is not possible given that the child is formula fed. Anal fissures are unlikely based a normal rectal exam. Allergic colitis should be considered but as a diagnosis of exclusion after all more seriour pathology is ruled out. Coagulopathy is also less likely given that this child demonstrates no other signs of bleeding, petechiae or bruising. I am also assuming that this child received Vitamin K at birth but again if she did not she would be demonstrating more signs of bleeding.
Based on your exam, the child is not toxic appearing but the PMD was concerned about hypotonia, abdominal distention and poor feeding, which definitely heightens my concern. For that reason, I would start with a two view abdominal x-ray, which would provide a lot of information about the bowel gas pattern and help think through other more concerning things on your differential including NEC, malrotation and hirschsprungs. Concurrently, I would also get a FOBT to ensure this is truly blood; a CBC to evaluate the extent of bleeding (and hold a blood culture in case); and coags to absolutely rule out a coagulopathy. If you had enough blood I might also consider a type and screen. I would defer a full sepsis work up at the beginning pending the results of your initial studies. I think it is appropriate to consult surgery as you did given her x-ray findings and begin a sepsis work up given her bandemia and worsening clinical status. As her x-ray demonstrates she likely has Hirschprungs but if it is resulting in hematochezia, it is likely secondary to enterocolitis and toxic megacolon, which definitely warrant antibiotics. Regarding antibiotic regimens I would give ampicillin, gentamicin and I would include flagyl for better anaerobic gut coverage.
Think Christina nails it for best/most comprehensive post! Only thing to add would be that I am skeptical an abdomen ultrasound has much role here. Two reasons:
1. The child is distended, likely gas (and your AXR confirms this) so your acoustic window will not be great.
2. It does little to rule in/out any of the differentials that Christina runs through. The one exception would be malrotation where you could look for the whirlpool sign and alignment of the mesenteric vein/artery. There is some literature re sensitivity/specificity for US in this setting, but I have not seen the surgeons also want the upper GI.
Christina covers it all there! Only thing to add – I am skeptical that US abdomen adds much here:
1. Belly is distended, likely gas (and your AXR confirms as much) so the acoustic windows will be terrible.
2. US does little to rule in/out most of the differentials set out by Christina./ The one exception is malrotation where you could look for the whirlpool sign and alignment of the mesenteric vessels. There is some data re sensitivity/specificity of this, but I have always had the surgeons want the upper GI regardless.
The differential above is complete, so my only thought about the case is the timing of the sepsis workup and antibiotics. The baby is well-appearing at the beginning. So a shared mental model with the team about holding on the sepsis workup initially can help keep the focus on getting labs and imaging. Then, when there is a tripwire– the baby looks ill, the imaging or labs are abnormal, then the team can reprioritize doing an LP and giving antibiotics.