
Hot Seat Case #115: 2 yo male with seizure
Posted on: August 20, 2018, by : Haroon Shaukat MD
Amie Cahill, MD Children’s National Medical Center
with Sabrina Guse, MD Children’s National Medical Center
2 yo previously healthy male arrived via ambulance after seemingly unprovoked GTC seizure-like activity. The family recently returned from summer trip abroad. They describe the episode as lasting a few minutes with eyes rolling back into his head. It resolved without intervention and he was sleepy for about 15 minutes then agitated for about an hour. No meds were given by EMS. No fever, no recent viral symptoms, no N/V/D, no headache, no other positive ROS.
Of note, 10 days prior to returning the patient fell backwards off a bicycle striking his occiput with brief LOC and immediate onset of seizure-like activity (GTC) lasting ~1 min then self resolved. He was cleared by his pediatrician there butsince then parents noted teeth grinding and myoclonic jerks while sleeping.
PMHx Negative. Born term, no complications. NKDA. UTD on vaccines. No medications. Growing and developing normally.
PSH: None
FHx: Negative. No cardiac disease, no sudden death, no epilepsy, no renal disease, no autoimmune disease, no genetic disorders
ROS: completely negative aside from what’s noted above.
PE:
VS: Temp 36.8 HR 90 RR 26 BP 100/66 O2 100% on RA
Weight: 12kg
GA: asleep, easily arousable, alert when awakened, interactive and smiling, WNWD
HEENT: NCAT, PERRL, EOMI, no nystagmus, normal conjunctiva, MMM, OP clear, TMs normal
NECK: supple, no TTP, trachea midline, no masses, no thyromegaly
CV: S1S2 RRR, no m/g/r, 2+ peripheral pulses, CR <2sec
LUNGS: CTAB, no w/r/r, no increased WOB
ABD: S/NT/ND, +BS, no HSM, no masses
GU: normal circumcised male genitalia
MSK: MAEW and symmetrically, no deformities
SKIN: no rash, no petechial rash, no ecchymosis
NEURO: Alert, oriented, CNs II-XII intact, 5/5 BUE/BLE strength, SILT, normal gait. NFDs
CT Head w/o contrast obtained and normal.
Patient remains well appearing, smiling, and playful in the ED. Results from initial workup: CBC normal, CMP Na 135 K 4.0 Cl 110 Bicarb 23 BUN 8 Cr 0.2 Glu 85 Ca. 5.1, albumin 3.6, LFTS normal, Phos 11.2, Mag 1.4.
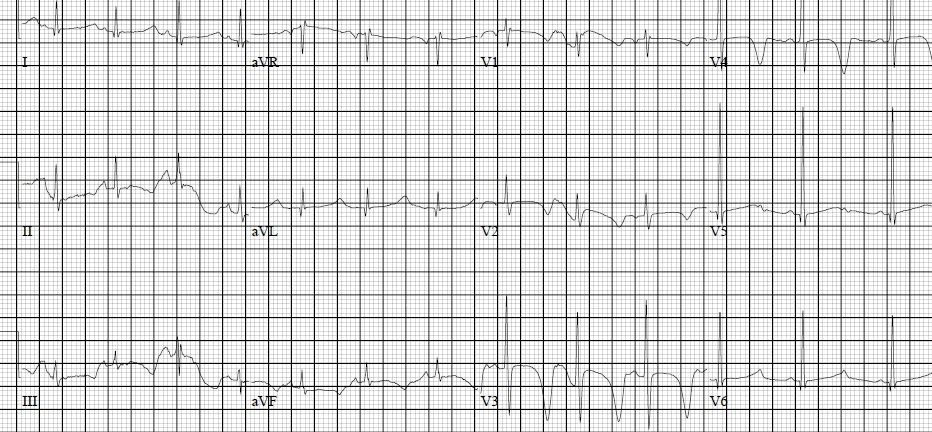
EKG as below:
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
While not the teaching attending for the week, just will make a few comments on this
1) Twists in the case are always welcome. Quite the twist with the Ca and Phos abnormalities. But that just goes to reinforce why we get screening labs for a variety of presenting symptoms….because there is a small chance that they could reveal something related to the underlying cause, if not the cause itself.
2) It always does befuddle me how many of these cases we see and just treat as “routine” and not get excited about. This is why we do what we do and enjoy our line of work so much (at least for me). On the flip side, even these “routine” cases (afebrile new onset seizure) are anything but routine for parents and that opportunity to empathize with the family and reassure them (which is usually possible) that we will work to understand and explain what’s going on is another driver for our enjoyment of this work.
3) While the hot seat polls are limited in how much we can ask, there’s always so much more and so many more things we can think to do, that any poll can really not capture all the possible options. This to me goes more to show how varied the art of medicine is, and how challenging it is to “teach” medicine when we all may do slightly different things/approaches to reach the same conclusion.
Just some food for thought. Looking forward to Thursday’s discussion.
Hm. What is going on here? I’m glad you chose to get screening labs on this patient, because those abnormalities are definitely concerning. My suspicion is that the teeth-grinding and myoclonic jerks have to do with the hypocalcemia, and the hypocalcemia is from the binding with excess serum phosphate.
But why is this phosphate so high? It doesn’t appear to be from kidney disease with a normal BUN and Cr, so I don’t think renal imaging is warranted at this time. Hopefully this is not a chronic issue; you’d suspect calcifications to appear on the head CT if this has been a long-standing issue. In addition with speaking with the neurologists, I’d be calling the endocrinologists for help on this one.
I calculated the QTc to be 610ms, which is definitely prolonged and puts this patient at risk for arrhythmias (did the patient initially syncopize instead of seize?). To me, this indicates a full loading dose of calcium gluconate (100mg/kg) and admission to the ICU for frequent checking of electrolytes. I find it doubtful that we could get this patient successfully admitted to the hospitalist team…
With low calcium, the child could be having tetany and seizures, as pointed out above. The prolonged QT and the risk for seizures makes treatment and closer monitoring in an intensive care setting warranted. The cause is most likely an endocrine disorder: DiGeorge and pseudohypoPTH would be distinguished from each other with a PTH level that is low in the former (parathyroid dysfunction) and high in the latter (body responds to low Ca by increasing PTH). Rickets is in the differential, but the child is old; limbs show no widening/flaring at the metaphyses; and the phos should be closer to normal. Discussion with Endo colleagues to assure that appropriate testing is done.