
Hot Seat Case # 117: 7 yo female with facial swelling
Posted on: September 20, 2018, by : Nadira Ramkhelawan
Nadira Ramkellawan, MD INOVA Fairfax Children’s Hopital
with Mike Falk, MD Children’s National Medical Center
7 year old healthy female brought in for tactile fever 4 days prior to arrival and periorbital swelling. The swelling began only on her right side which prompted an evaluation by her pediatrician. She was started on erythromycin ointment, zaditor, and benadryl with improvement in her symptoms. However the day prior to arrival she reported left eye swelling. She was evaluated at urgent care on the day of arrival, given ibuprofen for fever and zofran and referred to the ED for further evaluation. Patient reported pain on palpation of the left periorbital area and forehead. Denied pain with extraocular movements.
ROS: Decreased PO, 1 episode of NBNB emesis, no diarrhea, no weight loss. Denies change in vision.
PMH: None
PSH: None
PE: T 37.8 °C, HR 103, BP 113/68, RR24, SpO2 98 % on RA, Wt 54.9kg
General: appears tired but nontoxic. NAD
HEENT: NC/AT. Edema around the upper eyelids left > right. +tenderness on palpation of the forehead. No tenderness elicited over the maxilla. No conjunctival injection, no scleral icterus. Moist mucous membranes, oropharynx nonerythematous with no lesions.
Lymph: No cervical LAD.
CV: RRR no murmurs or rubs. Cap refill < 3secs.
Pulm: Good air entry bilaterally, no wheezing or crackles. No retractions
Abd: +BS, soft, NTND, no HSM
Neuro: Awake and alert, CN 2-12 intact, EOMI . Strength 5/5 in bilateral upper and lower extremities. Sensation intact and equal in bilateral lower extremities. No ataxia on ambulation or finger to nose. No cerebellar signs.
Skin: no rashes.
WBC 13.8 (62% neutrophils, 24% lymphs, 11 monos). ESR 72, CRP 9.8. blood culture pending.
CT maxillofacial obtained without contrast which showed frontal sinusitis, with possible subperiosteal involvement, as well as right maxillary sinus disease.
The patient was discharged home with afrin spray and augmentin PO. She returned to the ED 5 days later for new onset seizures. The father reported persistent fevers at home since being seen in the ED 5 days prior. Upon arrival, patient was actively seizing but the seizures self-resolved without medication.
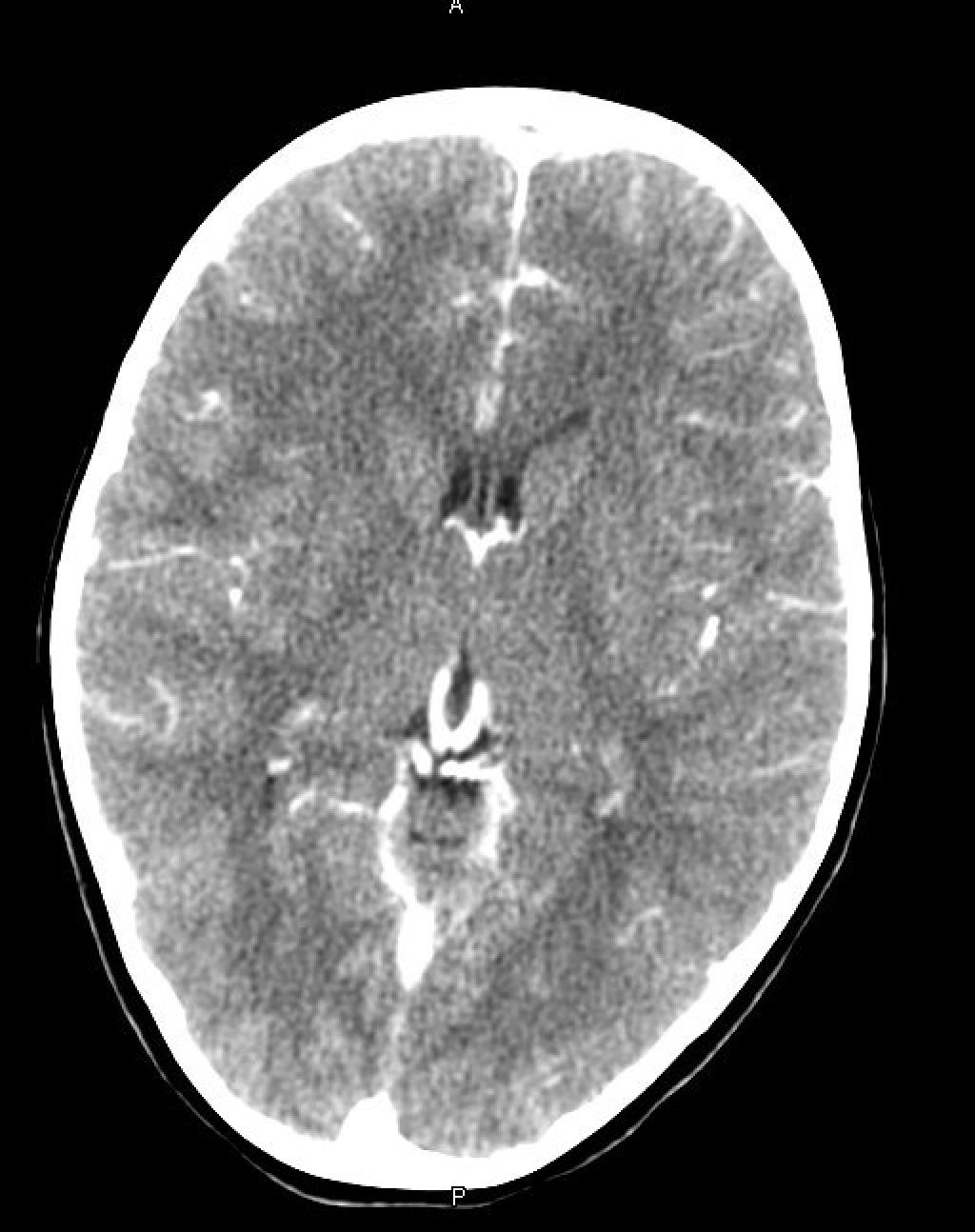
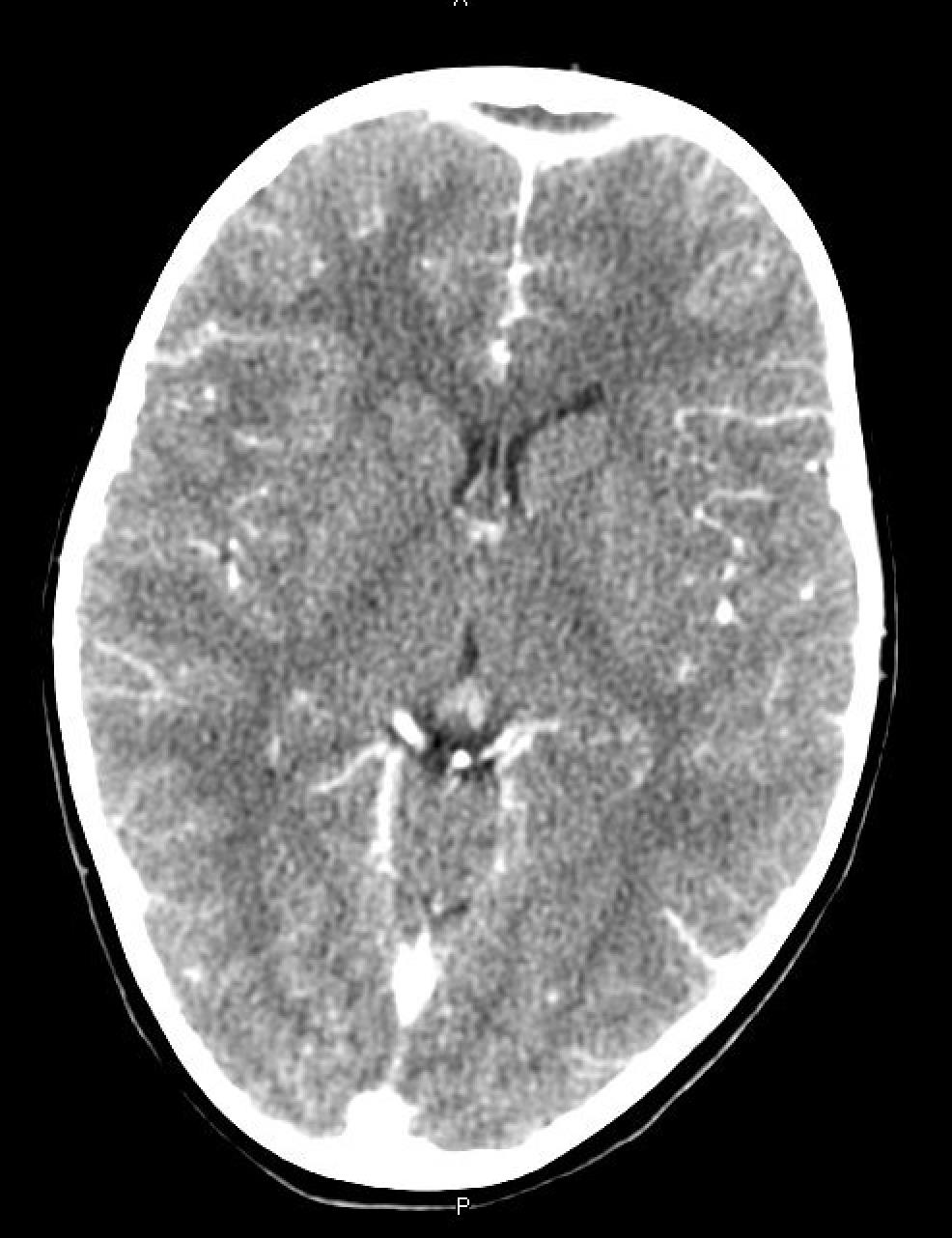
A CT scan of the head was obtained. Images below.


The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
At the risk of playing the role of Monday morning quarterback (technically it’s Tuesday as I write this…), I would have opted to admit the patient on the initial presentation. The WBC isn’t too crazy, but the elevated inflammatory markers with signs of subperiosteal involvement are concerning. The majority of subperiosteal abscesses arise from cases of sinusitis and/or orbital cellulitis. A quick literature review did not reveal a published standard of care for these patients, but a 2001 article in JAMA on the management of orbital subperiosteal abscesses found that all patients were admitted for IV antibiotics (and some for surgical drainage). Granted, the study was performed only at one institution, so it may not show the variability of practice in other hospitals around the country. However, the fact that 14 of 19 patients required surgical intervention makes me think that the risk of complications from SPAs is pretty high.
On second presentation, I would be pretty aggressive with antibiotic therapy and defer to the surgical colleagues on whether or not the patient would benefit from drainage of the evolving abscess that I can only assume are the etiology of the new seizure episode. I probably would not load the patient with antiepileptic drugs given that the seizure was self-limited, but having some benzos nearby wouldn’t be a bad idea…
In my mind, the most difficult decision for these children is to scan or not. I think once you pull that trigger, the further management decisions sort of uncover themselves.
If the patient was seen at onset (day 1 or 2 with only unilateral eyelid swelling, I probably would defer even though your exam reveals EOMI and lack of ophthalmoplegia). However, 4 days of fever with now bilateral eye swelling makes me feel uncomfortable with not scanning to look for orbital cellulitis 2/2 extension of sinusitis.
Interestingly, this patient doesn’t really seem to fit any of the diagnostic criteria for acute sinusitis: persistent nasal congestion/cough lasting >10 days, worsening of classic viral URI symptoms at days 5-7, severe onset and purulent nasal discharge for at least 3 consecutive days.
As an aside, what antibiotics do people prescribe if they are going to treat as an outpatient? Amox? Augmentin? Clinda? Cefdinir? Bactrim? A mixture of the above?