
Orthopedics- Upper extremity #1 discussion
Posted on: March 4, 2019, by : Haroon Shaukat MDJennifer Chapman, MD Children’s National Medical Center
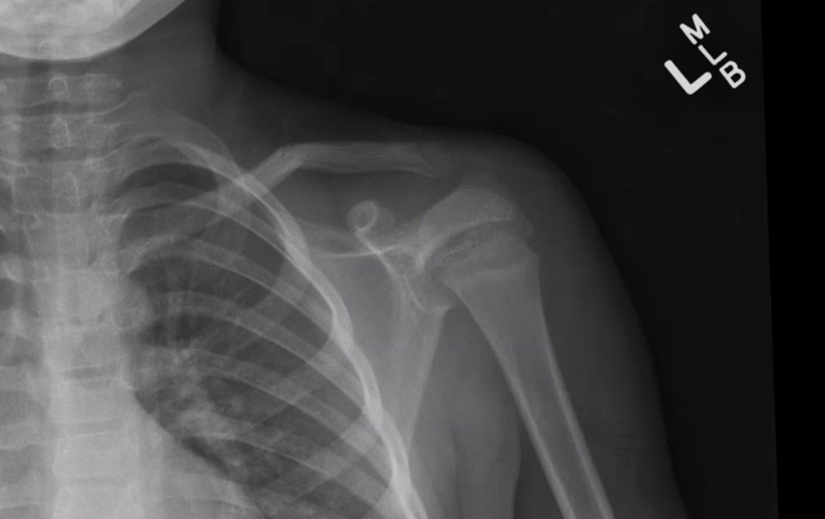
Case of a 12yo boy with upper chest pain after football collision.
Your responses:
Respondents: 4 PEM fellows and 2 faculty, no Associate/PA
Diagnosis: 7 votes –
No injury (0)
Fracture of clavicle (60%)
Other: R SC separation (12% )
Other: Sternoclavicular joint dislocation (28%)
Is Orthopedic consult needed in ED: Yes = 60% No = 40%
What treatment is needed:
Sling-and-swathe 33%
Figure-8-brace 17%
Reduction 50%
Our Orthopedic colleague responds:
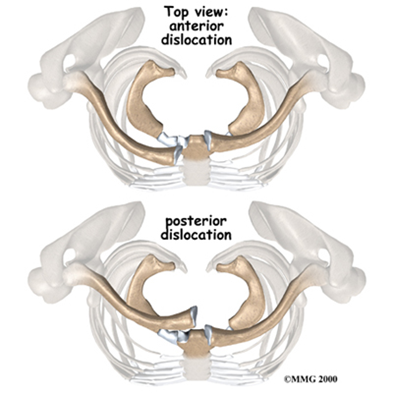
The diagnosis is right sterno-clavicular joint dislocation
Clinical Pearls:
1. On clinical exam, pain may be greater than expected with an apparently normal exam, or with only mild swelling over medial clavicular head.
2. The key is to think about this injury in the clinical context of a high-impact injury (contact sports, MVA) directly to the clavicle or to the shoulder, with translation of energy that causes the dislocation medially.
3. Stridor, dyspnea, dysphagia may suggest posterior dislocation and increases urgency of work-up. Why: structures behind the sternum:

4. This dislocation is sometimes difficult to visualize on a normal AP view of the clavicle. Obtain bilateral clavicles on the same exposure. Look for subtle asymmetry of the medial heads of the 2 clavicles. Usually, if the affected side is elevated, the dislocation is anterior. If inferior to the contralateral side, likely posterior. What does that look like structurally:
5. If this injury is suspected, obtain a serendipity view of bilateral clavicles. For this child:

Technique: radiograph beam is directed upwards at 40 degrees.
6. CT scan (or emergent MRI if available) is definitive for diagnosis of anterior versus posterior because plain film and clinical exam is never sufficient.
7. This can be a physeal fracture/dislocation of the medial clavicle, even into early adulthood but doesn’t significantly alter the management.
8. If reduction is planned, this should be accomplished in the OR with general anesthesia.
Red flags requiring Orthopedic consult in the ED:
1. Posterior dislocations/subluxations require orthopedic consultation in the ED.
2. If there is stridor, dyspnea, dysphagia, this may be emergent and thoracic/cardiothoracic surgery may even need to be called as backup by orthopedic surgery.
Pattern recognition: identify any injury





- Case 2- younger child with pain after a fall- R mid-clavicular transverse fracture with displacement. If skin is not tenting, no need for intervention or consultation.
- Case 2- 2 weeks later. Note the callus formation. There will be a firm round fullness as the callus forms and then slowly gets reabsorbed. Warn parents that they will see and feel a hard bump for several months.
- Case 3- school-aged child after a fall- Left mid-clavicular transverse fracture.
- Case 4- adolescent fall. L clavicular fracture with 3cm overriding segment.
- Case 5- 16yo boy after MVC with right sternoclavicular dislocation. There is a subtle asymmetry of clavicle heads that is somewhat more visible on serendipity view.
What remains unclear?