
Orthopedics- Upper extremity #2 discussion
Posted on: March 18, 2019, by : Jennifer Chapman
Jennifer Chapman, MD Children’s National Medical Center
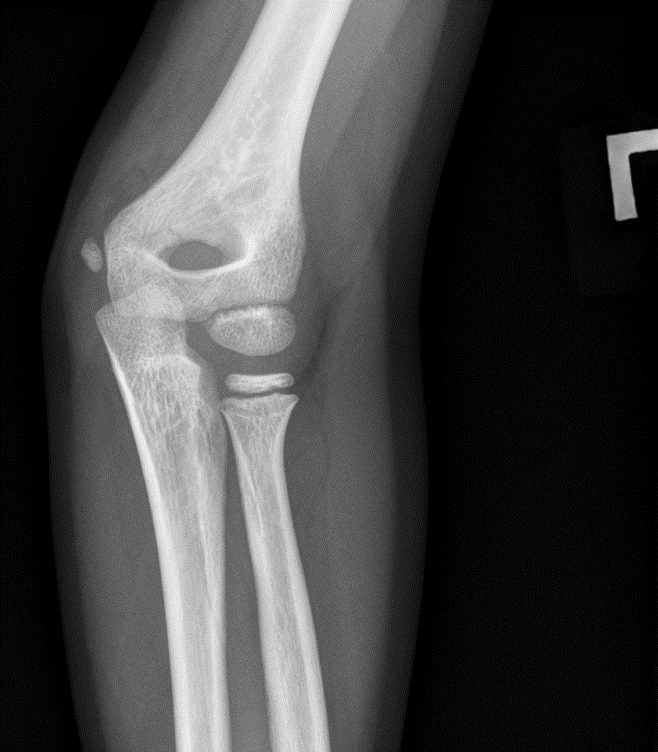
Case of a 2yo with a painful swollen elbow after falling out of bed.
Your responses:
Respondents: 9 PEM fellows, 1 NP, 3 Associates, 7 faculty
Diagnosis: 21 respondents
No injury 5%
Fracture of lateral epicondyle 60%
Type 1 SCFx with elbow effusion 20%
Radial neck fracture 10%
Other: Ulnar dislocation 5%
Is Orthopedic consult needed in ED:
Yes = 76%
No = 19%
Other: insufficient information without a true lateral 5%
Is Orthopedic consult needed in ED:
Yes = 76%
No = 19%
Other: insufficient information without a true lateral 5%
Our Orthopedic colleague responds:
The diagnosis is fracture of the lateral condyle of the left distal humerus.
Treatment: if non-operative, initial treatment is well-padded long arm posterior splint just past the wrist.
Clinical Pearls:
1. Diagnostic choices were intended to remind us that the epicondyle and condyle are different parts of the bone. What is the anatomy: a condyle is the rounded portion of the end of a bone articulating with another bone. There are medial and lateral condyles of both the distal humerus and distal femur. Lateral humerus condyle = capitellum and articulates with radius. Medial condyle = trochlea and articulates with ulna. The epicondyles are located proximal to each condyle and are points of soft tissue attachment – tendons and ligaments.

Capitellum – visible at ~ 1yo
Radial head ~3yo
Internal/medial epicondyle ~5yo
Trochlea ~7yo
Olecranon ~9yo
External/lateral epicondyle ~11yo

2. Mechanism and typical age: a fracture of the lateral condyle can be seen in all groups, from toddlers to adolescents. The mechanism is a fall, either on an extended hand or directly onto elbow.
3. On clinical exam, there is usually lateral swelling and even ecchymosis over the elbow or proximal forearm, and tenderness over the condyle, often laterally and posteriorly.
4. Diagnostics: Order 3 views of the elbow when assessing trauma. If a lateral condyle fracture is suspected, add an INTERNAL rotation oblique—the forearm is pronated at 45°. (this can be added into the comments of XR order in EMR). A medial condyle fracture is very rare, but if suspected, add an EXTERNAL rotation oblique.
5. Dispo: Many of these fractures are operative, even those that don’t look significantly displaced. For minimally displaced fractures, they may be hinged on intact cartilage and can be treated non-operatively in a cast but some are not hinged and are at risk for displacement, even in a cast.
6. Follow-up in 7-10 days is a reasonable timeframe, though some patients will be followed more closely to determine if there is displacement and consequent surgical pinning require
Red flags requiring Orthopedic consult in the ED:
Consult Ortho colleagues if the fracture line is visible and allow them to dispo the patient. Although these fractures are not necessarily indicated for emergent operative fixation, they have a unique set of complications, such as stiffness or permanent loss of elbow motion, late displacement, delayed or non-union, and rarely AVN.
Pattern recognition:












What is the injury:
Case 2- 4yo with lateral condyle fracture and elbow effusion. The oblique view is actually an external oblique, so different from what was discussed, but the fracture is well demonstrated.
Case 3- Toddler with lateral condyle fracture. Note how oblique view demonstrates the fracture more clearly.
Case 4- Early adolescent with lateral condyle fracture. The fracture fragment appears larger because the bone is more extensively ossified in this older child.
Case 5 – 6yo child with large elbow effusion and Type 1 SCFx.
Case 6 – 3yo with elbow effusion and lateral condyle fracture. Knowing ossification centers is useful when viewing the lateral radiograph, as the capitellum is visible along with an abnormal bony fragment.
What remains unclear?