
Orthopedics- Upper extremity #5 discussion
Posted on: April 29, 2019, by : Jennifer Chapman
Jennifer Chapman, MD Children’s National Medical Center
Case of a 5yo girl who fell and has forearm pain.

Your responses:
Respondents: 5 PEM fellows, 1 Associate, 9 faculty, 2 not categorized
Diagnosis options: (17 respondents)
- Proximal ulnar fracture 6%
- Elbow effusion Type 1 SCFx 0
- Radial neck fracture with elbow effusion 23%
- Forearm fracture with elbow dislocation 6%
- Deformity of ulna with wrist dislocation 41%
- Normal 6%
- Other, describe: radial head dislocation 18% partial credit!
Diagnosis: this was initially read as normal. There is a plastic deformity of the ulna with dislocation of the proximal radius, a combination called a Monteggia fracture.
Our Orthopedic colleague responds:
Clinical Pearls:
1. The do-not-miss injury is the radial head dislocation. A good lateral view of the elbow or forearm is needed to know that the elbow is correctly aligned. There are 2 alignments systematically reviewed when looking at a lateral forearm or elbow radiograph:
i) The first is that the long axis of the radius always points to the capitellum, no matter what age (and actually no matter what view). On a good lateral view, the anterior humeral line should intersect the capitellum in the middle to anterior third. Malalignment indicates a radial head and/or a frank elbow dislocation.
ii) The second alignment is that the anterior humeral line should intersect the capitellum in the middle third. Malalignment helps in the diagnosis of type 2 and 3 supracondylar fractures.

In the fracture case, the radius points above (or ‘volar’ to) the capitellum, leading to the diagnosis of a radial dislocation that must be reduced.
2. When reviewing a radiograph, how does one know that the lateral view is adequate? Look for these 3 findings:
– you can see the radiocapitellar space and the ulnohumeral space well;
– the anterior cortex of the distal humeral shaft is a straight line down (not curved) until it terminates at the condyles.
– the ‘hourglass’ of the distal humerus is apparent. The hourglass is made up of the outlines of 2 fossae (shallow depressions) of the distal humerus: the coronoid fossa in front and the olecranon fossa in the back of the bone:
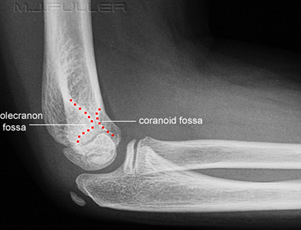
Putting it together, look at this normal lateral elbow Xray to see these 3 findings:

3. The ulnar fracture is called a ‘plastic bowing deformity.’ This occurs primarily in the younger pediatric patient, in whom the flexible bone deforms with an axial load but then fails to spring back to its original position. Because there is actual deformity, this often needs to be corrected. In this case, manipulation is needed at the time that the radial head is reduced.
4. The combination of an ulnar fracture with a radial dislocation is called a Monteggia fracture. It is not common, but when seen, usually involves a transverse fracture of the proximal ulna. The key is to see the dislocation.
Red flags requiring Orthopedic consult in the ED:
1. This is not a fracture that can be splinted and followed up in several days. This should generate an orthopedic ED consultation as it can be associated with a posterior interosseous nerve palsy and delay in care can cause considerable morbidity, including loss of elbow motion and nerve injury.
Pattern recognition:







Pattern recognition:
Case 2: this is the Monteggia pattern: there is a proximal 1/3 ulnar fracture (oblique in this child), with a malalignment of the radial head and the capitellum, indicating a proximal radius dislocation.
Case 3: transverse fracture of the proximal ulna, with comminution and with a longitudinal component extending to the tip of the olecranon. The radius is in the correct position. So this is an isolated ulnar injury.
Case 4: fracture of the proximal ulna. The head of the radius seems to be well aligned. The arrow drawn along the long axis of the radial bone runs just superior, or volar, to the capitellum, indicating that there is, in fact, a radial dislocation. This is a Monteggia fracture.
Please share any points that remain unclear.
Thank you, I just returned from a mission in Haiti and we saw a child with this fracture, we identified it with US.
Very helpful to understand the fracture, and treatment. I really appreciate the pattern recognition.
Thats great!