
Push-Pull Fluid Bolus in Pediatrics
Posted on: April 8, 2025, by : Haroon Shaukat MD✅ Indications for Push-Pull Bolus:
- Pediatric septic shock
- Hypovolemia (trauma, dehydration, hemorrhage)
- Rapid fluid resuscitation during code situations
- Poor perfusion with hypotension
Typical Fluid Dose:
- 20 mL/kg isotonic crystalloid (Normal Saline or Lactated Ringer’s)
- Repeat boluses as clinically indicated (up to 60 mL/kg initially in septic shock)
Push-Pull Technique Using a 3-Way Stopcock
Equipment Needed:
- 60 mL syringe
- IV fluid bag (NS or LR)
- 3-way stopcock
- Extension tubing connected to the patient’s IV line
✅ Steps to Set Up:
- Connect the 3-way stopcock:
- Port A: IV fluid bag via IV tubing
- Port B: 60 mL syringe
- Port C: To the patient’s IV
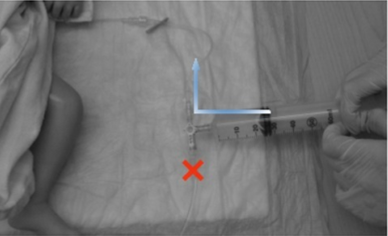
- Turn the stopcock OFF to the patient.
- Pull back the syringe to draw fluid from the IV bag.
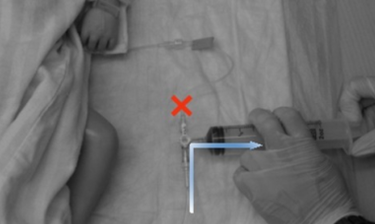
- Turn the stopcock OFF to the IV bag.
- Push fluid from the syringe directly into the patient.
- Repeat: Alternate between drawing fluid and pushing to patient until desired bolus is delivered.
✅ Pro Tips:
Keep the IV site visible—stop immediately if infiltration is suspected.
Use the largest-bore IV possible for effective flow rates.
Limit disconnections to maintain sterility and prevent air embolism.
Monitor for signs of fluid overload—rales, hepatomegaly, worsening work of breathing.
🔗 Video Demonstration of Push-Pull with Stopcock:
Push-Pull Bolus Method – Children’s Colorado
💡 Alternatives to Push-Pull:
Rapid infuser device (if available)
Pressure bag (less controlled than push-pull)
Syringe pump (slower for large volumes)